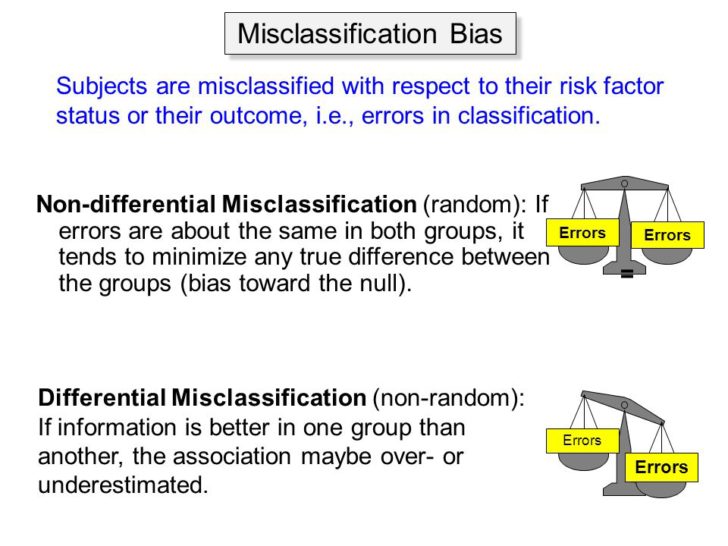
A great example of differential misclassification bias that was a criticism of the secondhand smoke epidemiology — i.e., smokers pretending they were nonsmokers. Here’s a quantification of the effect.
Wow…
More than 40% of those 822 self-reported quitters failed the saliva test.
The media release is below.
###
Smokers in clinical studies who say they’ve quit often haven’t
SOCIETY FOR THE STUDY OF ADDICTION
A new US study published by the scientific journal Addiction has found that a high proportion of smokers enrolled in stop-smoking programs during a hospital stay report having quit when in fact they have not. The findings mean that in these kinds of study it is vital to check claims of having quit using an objective measure.
This nationwide study followed five large smoking cessation clinical trials in the US that enrolled smokers at hospitalization. At 6-month follow-up, 822 participants (out of 4,206 who completed the follow-up survey) reported they had not smoked in the past 7 days and provided a usable saliva sample for verification by testing for a chemical called ‘cotinine’. The liver converts nicotine in the body to cotinine and so this chemical is a very accurate measure of whether someone has smoked in the past few days. More than 40% of those 822 self-reported quitters failed the saliva test.
The misreporting rate may be even higher because, despite the offer of $50 to $100 for providing a sample 18.6% of people who had said they had quit smoking did not reply, even after multiple attempts. These participants were excluded from the study. The study also excluded anyone who said they were using another nicotine product such as smokeless tobacco, nicotine patches or e-cigarettes. Even very heavy exposure to other people smoking would not have raised cotinine levels to those found in this study.
Lead author Dr. Taneisha Scheuerman says “Our study shows that in studies where participants may feel pressure to say they have quit when they have not, it is essential to verify claims of quitting using an objective test such as cotinine to know true quit rates. For clinical researchers, another important finding is that misreporting rates were similar across intervention and control conditions, suggesting that the relative effectiveness of interventions tested was the same using self-report and cotinine levels.”
Professor Robert West, Editor-in-Chief of the journal, Addiction, that published the article comments, “Other research has shown very low misreporting rates in population surveys of smoking. Hospital patients and pregnant women would be likely to feel strong pressure to have stopped smoking.”
###
Further verification of the Dr. Gregory House Principle — “Everybody Lies.”
Given the large surcharge on smokers in the current insurance market in the US, there is a large incentive to lie. Also since the medical records are all electronic these days, people assume that there is little privacy. So there is a strong incentive to lie, and to refuse to be tested in case it affects their insurance rates. Providers should be able to tell by the smell. I have noticed that many PA’s seem to chew gum while seeing patients. I suspect that this is to hide their own smoky smell!
Tadchem, the people running these studies though often have more than enough money to at least partially compensate for both sources of bias. They can get a truer population to participate by offering more money, and they can check on lies by offering a sizable bonus at the very end to any participant willing to undergo a spit/blood/hair test for CO and/or cotinine. The participants can be strongly reassured that accepting the extra money will not in any way penalize them if the results show they lied. The names could even be blinded.
Even if a few STILL opted out, the researchers could take their final results and say, “At worst, all five of the refusing subjects were actually secret smokers, and if so then that would have had X%ish effect on our findings.” (Heh, you MIGHT occasionally get a nonsmoker who wanted to pass off as a smoker, but that’d be pretty rare unless they were trying to sue the tobacco companies! LOL!
Bill,
I think you may have something there…
The two fatal and irreparable flaws in polling, whether for demographic studies or any other statistical surveys, are that some people will not participate (the ‘opt out’ demographic) and some people, for whatever reason, choose to lie. There is no known way to compensate for these sources of bias.
Hmm… odd that the Journal seems so willing to jump on the large effect misclassification has on studies about smokers quitting… but has always been almost silent on the effect such misclassification has on secondary smoke exposure and disease studies.
When Hirayama’s “Japanese Wives” study came out ca. 1980, it almost totally ignored the magnitude of the effect in the restrictive culture that frowned heavily upon “proper” women smoking cigarettes. Even a moment’s thought would bring a neutral observer to the the realization that such prejudice would strongly encourage misreporting; and a second moment’s thought would point up the likelihood that such “secret smoking” might be far more likely among women married to smokers (both in terms of easy availability of stolen cigs and in terms of the male spouse not realizing that his wife had the occasional scent of tobacco around her.
Given the extremely strong association claimed between even low levels of social/occasional/secret smoking and lung cancer, associations indicating an increase of literally hundreds of percent, such an oversight would seem to be truly incredible, no?
One could try to explain it by saying the motivations behind Hirayama’s and many other such studies in overlooking such things are deliberate and designed to further the social engineering attack on smoking that fear of secondary smoke exposure has allowed.
That would not be nice however.
Perhaps someone out there could offer a nicer explanation?
– MJM
They may be telling the truth. Lots of smokers have “quit”—many times.
Rog. L, you think that might have something to do with political polling results too?
“Hospital patients and pregnant women would be likely to feel strong pressure to have stopped smoking.” [Therefore more likely to give what they thought to be the ‘required’ answer i.e. reported as having quitted….]
The vast majority of self-reported personal information must be assumed to be biased in the direction the ‘self-reporter’ sees as being required by the ‘authority’ or ‘experts’ conducting the survey………. e.g.;
Is your income over $1M?…………’Yes’
Is your car > 1 year old?……………. ‘No’
Do you ‘do it’ more than twice daily?……..’Yes’
Of course trying to quantify this bias would be practically impossible………..