… even though one of its cited “experts” tacitly admits there is no established cause-and-effect relationship between typical/normal/current salt intake and adverse health effects.
WebMD reports:
The [Institute of Medicine’s recommendations for population wide reductions in salt inane] are welcome, according to Suzanne Steinbaum, DO, director of women and heart disease at Lenox Hill Hospital in New York. “For 40 years, we have known the correlation between salt intake and its negative effects on the body, but it has been an almost impossible goal for Americans to reduce their salt intake to only what is considered adequate.”
It is, of course, Statistics 101 that a “correlation” cannot establish cause-and-effect — so if no cause-and-effect has been established after decades of intensive research on dietary salt, why would anyone follow recommendations based on nothing?
Check out these 10 Myths about dietary salt compiled by Dr. Mort Satin of the Salt Institute:
MYTH 1:
We eat more salt today than ever before.
FACT: Our current salt consumption (1.5 to 1.75 teaspoons per day) is about one half of the amount consumed between the War of 181213 and the end of World War II,14 which was about three to 3.3 teaspoons of salt per day.
MYTH 2:
Our knowledge of the major sources of salt in our diet (i.e., 80 percent from processed foods) is unquestionable.
FACT: These data referred to in every medical publication is based on a single paper from 1991, which involved a dietary recall (a very unreliable method of data gathering) of a total of just sixty-two persons.15
MYTH 3:
Our salt consumption continues to rise every year.
FACT: There has been no change in our consumption of salt since the mid-1950s.16
MYTH 4:
The thirty-year public health initiative in Finland represents a successful model of salt reduction.
FACT: While Finland was able to reduce salt consumption among its population from 2.3 teaspoons of salt per day down to 1.3 teaspoons per day in the period from 1970 to 2000 (in much the same way that the U.S. did from 1945-1960), the health benefits that they have achieved during the same time period were no better (and, in fact, marginally worse) than neighboring and other countries that did not reduce salt consumption.
MYTH 5:
Current levels of salt consumption result in premature cardiovascular disease and death.
FACT: When average life expectancy in various countries is plotted against the average salt intake in those countries, it is clear that the higher the salt consumption, the longer the life expectancy. (See Figure 3.)
While no cause-and-effect relationship between sodium intake and lifespan is implied, the data clearly demonstrate the compatibility between life expectancy and the associated levels of sodium intake.

MYTH 6:
Cutting back on salt will improve the overall diet.
FACT: Salt makes the bitter phytochemicals in salad greens and vegetables more palatable. Removing salt from dressings or accompaniments will make these important diet items less acceptable and will discourage people from eating them.
MYTH 7:
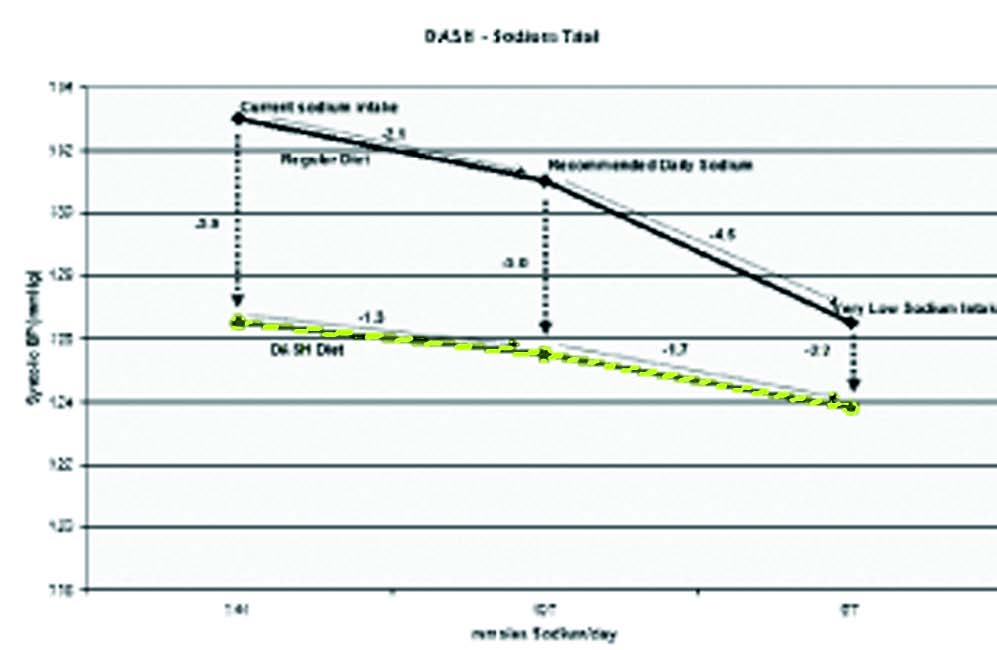
Reduced salt levels are critical to the DASH diet.
FACT: When the results of the DASH Sodium trial are examined (see diagram in Figure 4), it is immediately apparent that merely moving to a DASH diet (red line) has a significantly greater impact on blood pressure than simply lowering salt consumption. Dropping from the normal level of sodium consumption to the Dietary Guidelines’ recommended level reduced the systolic pressure in the American diet (blue line) by an average of 2.1 mm Hg. However, simply changing from a standard American diet to the DASH diet, without any changes to sodium consumption, reduced the systolic blood pressure by 5.9 mm Hg, almost three times the drop resulting from the recommended sodium reduction. More important, reducing salt makes the DASH diet far less palatable and thus discourages people from adopting it.
MYTH 8:
There is a clear relationship between salt intake and blood pressure.
FACT: The lack of a clear relationship between salt intake and blood pressure is best exemplified with the standard hospital saline IV drip, which supplies an average of three liters of 0.9 percent sodium chloride per day. This is equivalent to twenty-seven grams of salt (4.5 teaspoons) per day while in the hospital in addition to the six grams (one teaspoon) of salt taken in food (if the Guidelines are followed). That is a total of thirty-three grams of salt per day or more than five times the Dietary Guideline recommendations! Yet patients’ BP is checked every four to six hours and does not change. Where is the purported relationship of salt intake to blood pressure?
MYTH 9:
Reducing salt intake can do no harm.
FACT: Reduced salt intakes have repeatedly been linked in the medical literature to the following conditions:
• Insulin resistance (diabetes)
• Metabolic syndrome
• Increased cardiovascular mortality and readmissions
• Cognition loss in neonates and older adults
• Unsteadiness, falls, fractures
• Lifelong avidity for salt
• And more
MYTH 10:
The U.S. Dietary Guidelines process is valid.
FACT: The original Dietary Recommended Intakes (DRI), issued under the imprimatur of the Institute of Medicine (IOM) (National Academy of Sciences), were immediately accepted internationally and spared the critical scientific review normally given to nutritional recommendations. Indeed, any conscientious perusal of the document reveals the numerous compromises and rationalizations made in lieu of actual evidence in order to arrive at the final recommendations. This was reiterated during a 2007 IOM workshop entitled, “The Development of DRIs 1994–2004: Lessons Learned and New Challenges,”17 where several participants stressed that the DRIs were largely based on the lowest quality of information—opinion—rather than on randomized controlled clinical trials which represent the highest quality of evidence. Yet the disposition of the DRIs provides an insight into how far we have strayed from the scientific principle of adherence objectivity and evidence-based medicine.
The five-year Dietary Guidelines for Americans (DGA) review process has always been publicized as being an “independent and objective” reevaluation of the previous DGAs. The 2005 DGA for sodium referred to the DRIs as a foundation document and assumed all its recommendations. The consequent 2010 DGAs reconfirmed the recommendations of the 2005 DGAs with the proviso that the at-risk populations consume 1,500 mg sodium per day for the upper limit. As it happened, the Chair of the original DRIs committee that set the first recommendations for sodium also happened to serve as the Chair of the 2005 Dietary Guidelines Subcommittee on Electrolytes and thus evaluated the very recommendations that he was responsible for promulgating in the first place.
In 2010, the process was repeated and, once again, the same Chair of the Subcommittee on Electrolytes ran the show. This sequence, fully sanctioned by the Institute of Medicine and the U.S. Department of Agriculture, begs the question as to whether any “independent and objective” analytical process can feature a single individual piloting the creation of standards (DRIs) who then is charged with evaluating his own recommendations five years later, and asked once again to evaluate his prior evaluations. This process makes a sham of the concept of independent, objective evaluations and makes a mockery of the integrity of our great scientific institutions!
WebMD – the place for ‘science’. Am I right?
“Not getting enough salt can kill you.”
Isn’t that the goal of all of the food Nazi’s “recommendations”? If it doesn’t end your life prematurely, it will make you wish you were dead.
For example, I am type II diabetic. As an engineer, I did a process control study on what was required for ME to have normal blood sugars. It turned out to be quite the opposite of what the American Diabetic Association was recommending. If I had followed their advice, I would likely be dead by now or at least blind and a multiple amputee.
As it is, I have had normal blood sugars since shortly after I was diagnosed (ca. seven years ago) and without the usual side effects of an uncontrolled blood sugar level. As a consequence, I can safely relax my initial very restricted diet and still maintain normal blood sugars. My original diet was no naked carbohydrates (sugar, honey, pastries, bread, pasta, root vegetables and the like). I ate mostly leaves, stems, cinnamon flavored sawdust and restricted quantities of pinto beans, chicken, beef, nuts, red raspberries, peanut butter, and high fiber crisp bread.
My conclusion is that the food Nazi’s don’t have a clue about what it is they pretend they know. Their goal is to exert power and control over those who know even less than they do and not to worry about the consequential body count.
Reduced my salt intake and it almost killed me. My blood pressure has always been 120/80. Several years ago I started reducing my salt intake because everyone including Mayor idiot Bloomburg were constantly preaching lower salt. My blood pressure slowly lowered to 100/60. During an all day all terrain vehicle ride I passed out, slumped forward, pressed the thumb throttle to full power and rocketed over a banked turn and into a desert tree at full speed. Luckily the tree caught the ATV and I landed in soft river bottom sand with a severe rotational concussion and minor scratches and bruises. Helicopter ride, emergency room and every test possible ended with my heart doctor looking at me and saying, “I think you just need to eat more salt”. Started adding salt to my gator aid and got my blood pressure back up to 120/80. Don’t get light headed and feel much better.
Not getting enough salt can kill you.
Reblogged this on Petrossa's Blog and commented:
Salt,sugar, fat, you name it and there is someone making the correlation/causation error, creates a hype and makes life miserable for the gullible. In the past salt was a conservation agent, everything was salted to a point we today couldn’t eat for its extremely salty taste. Still humanity managed to survive and reproduce.